



“My daughter Rubi is only 13 months old and falls sick very often. She is too small to take any home-cooked food. I continue to breastfeed her, and she takes some snacks like Pipe Fryums (Yellow Ponga), mixture, chips, kurkure, etc., from the local shop. The Anganwadi Didi has asked me many times to take Rubi to the Govt. Nutrition Rehabilitation Centre (NRC). She says that my daughter Rubi is underweight, but I cannot leave my household work and go for two weeks to NRC,” Nanhi Anuragi.
Nanhi Anuragi is one among many women in Chhatarpur district, Madhya Pradesh, struggling with childhood malnutrition. According to the POSHAN District Nutrition Profile, Chhatarpur consistently ranks among the highest-burden districts in the state. In 2020–21, the prevalence of underweight children under five was 34.6%, higher than the Madhya Pradesh average of 33.0%.
Malnutrition remains a major public health concern across India. Undernutrition in children under five is associated with impaired physical growth, cognitive delays, and increased susceptibility to infections and illness.

Evidence shows that community-based management of acute malnutrition is highly effective. Nearly 80% of children with Severe Acute Malnutrition (SAM) can be treated at home, provided they receive timely care, counselling, and follow-up.
NERS: A Community-Based Response
The Comprehensive Primary Health Care Project (CPHCP) of Bethesda Hospital Society works closely with the public health system to improve service quality and nutrition outcomes for under-five children in Nowgong block, Chhatarpur district. To address malnutrition, the project mobilised communities to organise Nutrition Education Rehabilitation Sessions (NERS) in six villages. Locally, the initiative was named “Bal Suposhan Shivir” (Children’s Nutrition Camp).

NERS aims to improve the nutritional status of malnourished children by strengthening knowledge, attitudes, practices, and skills (KAPS) of mothers and caregivers related to child feeding, hygiene, and care. The module, developed by the Community Health Department of the Emmanuel Hospital Association (EHA), aligns with the Sneh Shivir approach of the Integrated Child Development Services (ICDS).
Sneh Shivir is a community-based initiative under the ICDS mission in India, designed to address moderate and severe undernutrition in children. These camps facilitate “learning-by-doing” for mothers on nutrition, hygiene, and feeding behaviors and are organized for 12 days in selected Anganwadi Centres (AWCs) with high rates of malnutrition, often involving a “cluster approach” where one AWC serves 4-5 nearby centres. The modules and activities within Sneh Shivir are designed to promote positive care practices around feeding and hygiene through behaviour change, utilizing a “Suposhan Kunji” (Nutrition Handbook) and a series of nutrition-health education sessions. It aims to engage parents, children, and caregivers in community-based nutrition rehabilitation.

Structure and Training Design
NERS is a 12-day intensive programme for mothers or caregivers of under-five malnourished children. Sessions are held for about three hours daily (11:00 am–2:00 pm), with timings decided by participants to accommodate household responsibilities. Learning is participatory, combining discussions with demonstrations and hands-on practice.
The training design was adapted to local needs:
- Village-based rather than cluster-based
- Focused on locally prevalent child health conditions
- Emphasised home-based fortnightly follow-up instead of centre-based care
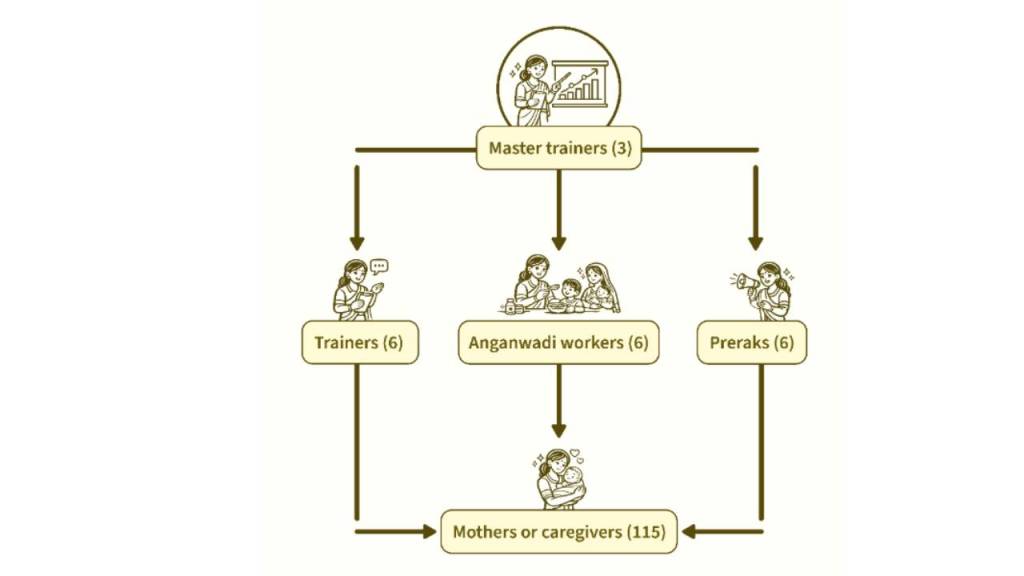
Training was conducted at three levels:
- A three-day Training of Trainers for the CPHCP team and Community Coordinators
- A two-day orientation for Anganwadi Workers (AWWs) to support demonstrations
- A two-day training for village Preraks to strengthen mobilisation and follow-up
Implementation and Outcomes
A weighing campaign across Maharajpur and Kurraha PHCs identified six high-burden villages. Community awareness was generated through wall writings and household mobilisation. Sessions were conducted in August–September 2025 with the involvement of Panchayat Raj Institute (PRI) members.
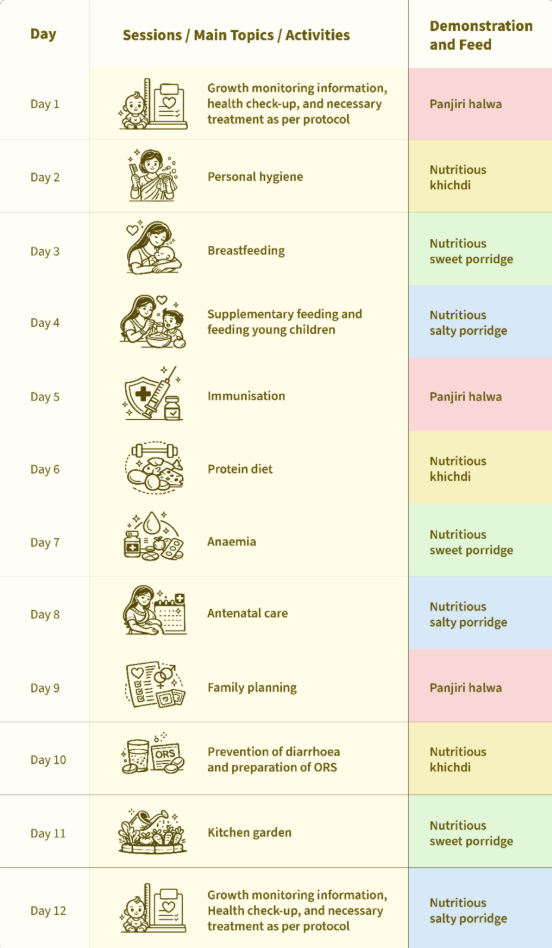
On Days 1 and 12, ANMs re-screened children, recorded baseline measurements, and conducted health check-ups. Six children with SAM and medical complications were referred to higher centres. Four were admitted to the Nutrition Rehabilitation Centre (NRC) at Chhatarpur District Hospital, and one to Maharajpur PHC. Other children received Vitamin A and deworming. The deworming was repeated after two weeks.

A total of 115 children participated, with 86% (100 nos.) caregiver attendance across all 12 days. Mothers brought locally available ingredients to prepare nutritious mixes, including high-protein foods. Feeding practices, hygiene, and handwashing were demonstrated and practised daily.

By Day 12, the average weight gain was 278 grams per child. Over the next three months, fortnightly home follow-ups showed an average weight gain of 845 grams.
Key Observations
- Improved caregiver knowledge, attitudes, and feeding practices
- Increased use of locally prepared nutritious foods
- Reduced junk food consumption
- Improved hygiene and handwashing habits
- Better utilisation of Anganwadi nutrition supplies
- Increased proactive identification of malnutrition by AWWs
- 24% reduction in underweight and 36% reduction in wasting within 12 days
Encouraged by these outcomes, ICDS officials have recommended scaling NERS to other villages.
Looking Ahead
The NERS experience demonstrates that coordinated government–NGO efforts, grounded in community participation and caregiver empowerment, can significantly reduce childhood malnutrition. Building on this success, plans are underway to expand the programme to more villages—ensuring many more children are protected from the long-term consequences of malnutrition.

“My daughter Rubi has started eating home-cooked food and I have stopped giving her junk food. I never believed that she could gain weight by 300 grams in just 12 days. We’re thankful to the entire project team for their tireless efforts to train us in taking care of our malnourished children in our village itself”, said Nanhi Anuragi.